The most common therapeutic method for early stage distal esophageal cancers and proximal stomach
cancer is surgery. One of the challenges in esophageal surgery is to maintain gastrointestinal continuity.
The neoesophagus is transferred from the posterior, mediastinal, or retrosternal areas to the cervical
region. A 61-year-old male patient with esophageal cancer had received transhiatal total gastrectomy,
distal esophagectomy, and Roux-en-Y esophagojejunostomy. Right thoracotomy had been performed due
to anastomotic leak with the esophageal stump left behind. Left thoracotomy and metastasectomy were
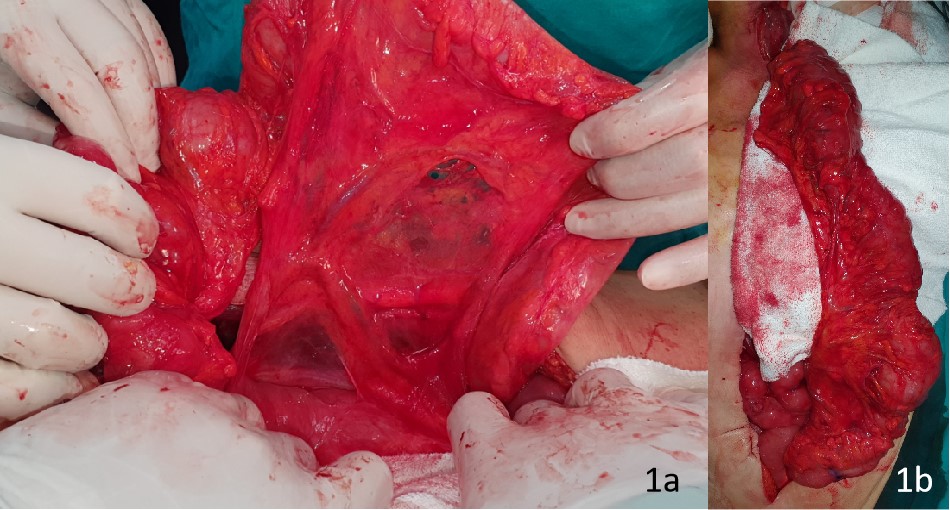
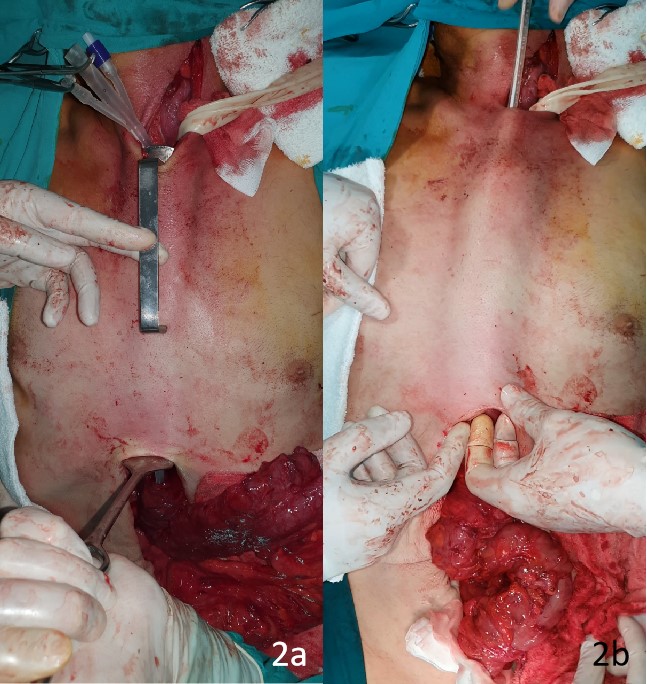
also performed due to lung metastasis. The left colon was transpositioned from the presternal area to
the cervical region for reconstructive purposes. Physicians should bear in mind that the conduit can be
advanced in the presternal area as the last resort for its localization in esophageal surgery. The aim of this
study was to present, along with literature review, the case of a patient with distal esophageal cancer for
whom presternal colonic transposition was performed with the es ophageal stump left behind.
Download Citation: Endnote/Zotero/Mendeley (RIS) RIS File
Download Citation: BibTeX BibTeX File