\n Amaç: Stres üriner inkontinans tedavisinde yaygın olarak kullanılan Trans Obturator Tape (TOT) uygulamalarında eksizyon gerektirecek meş erozyonları gelişebilmektedir. Çalışmamızda TOT uygulamasına bağlı oluşabilecek üretral meş erozyonunu önleme amaçlı olarak geliştirdiğimiz subüretral sling altına yerleştirilen vajinal flep yöntemini tanımladık ve hastaları postoperatif komplikasyonlar açısından değerlendirdik.
\n
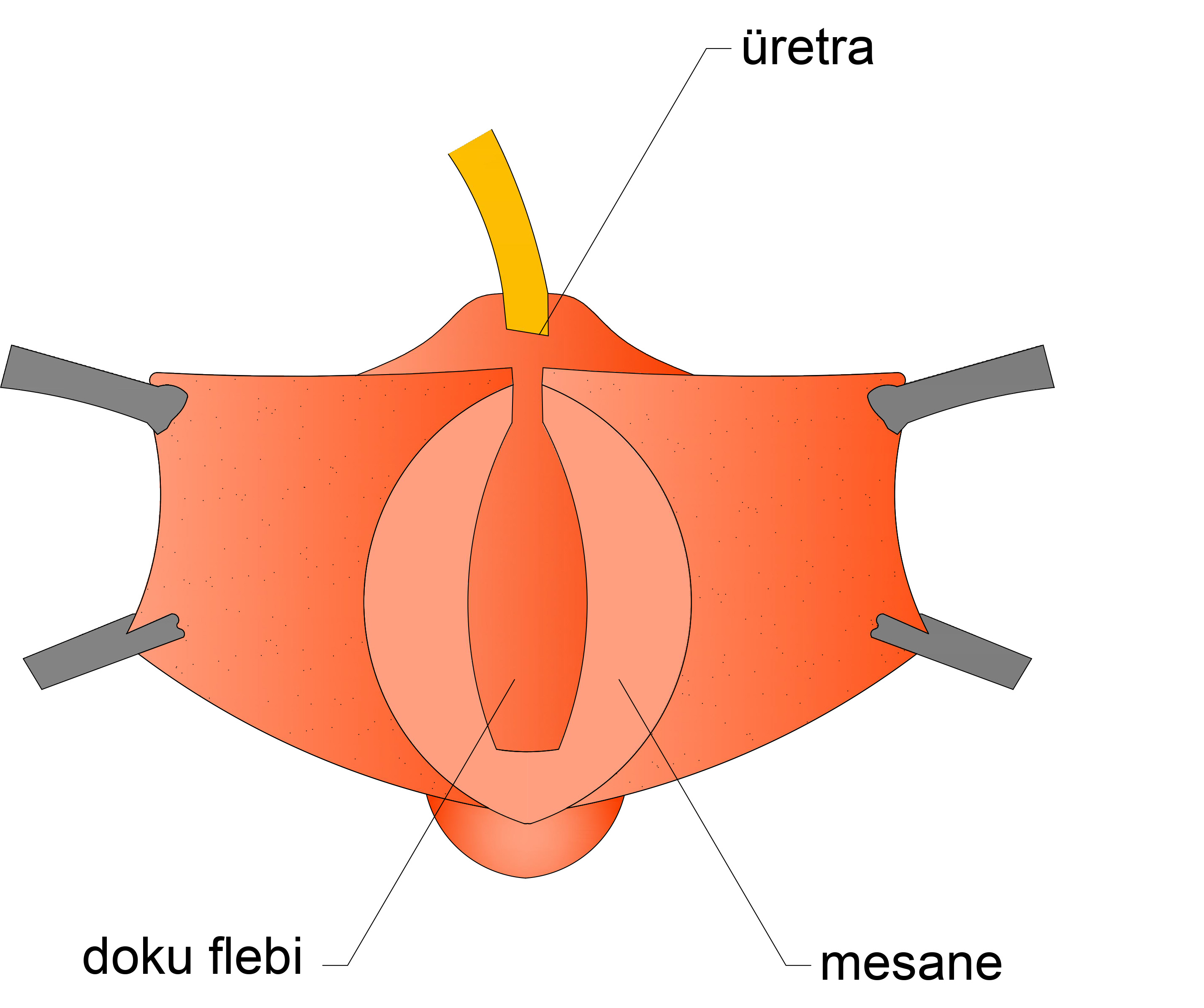
\n Gereç ve yöntemler: Çalışmamızda Aralık 2014 ile Mayıs 2018 yılları arasında hastanemizde aynı seansta TOT ve sistosel operasyonu olan ve vajinal mukozadan oluşturulan flebin üretra önüne ve meş altına yerleştirildiği 22 hasta retrospektif olarak incelendi. Hastalar üretral meş erozyonu, vajinal meş erozyonu, urgency ve disparoni şikayetleri, üriner retansiyon ve ikincil cerrahi gerekliliği açısından değerlendirildi.
\n
\n Bulgular: Hastaların postoperatif ortalama takip süreleri ortalama 8,95±8,45 aydı. 20 hastaya aynı seansta TOT ve sistosel operasyonu (%90,9), 2 hastaya aynı seansta vajinal histerektomi, TOT ve sistosel operasyonu (%9,1) uygulanmıştı. Takip süresi boyunca hiçbir hastada üretral erozyon gelişmedi. Sadece aynı zamanda menapozda olan bir hastada vajinal mesh erozyonu ve disparoni şikayeti vardı. Başka bir hastada üriner retansiyon ve taşma inkontinansı gelişti. Bu hastaya aynı seansta vajinal histerektomi, TOT ve sistosel operasyonu uygulanmıştı. Bu hastaya daha sonra meş kesilmesi işlemi uygulandı.
\n
\n Sonuç: Vakalarımızda uygulanan cerrahi teknik ortalama 9 aylık yakın dönem takipte üretral erozyondan tümüyle korumasının yanı sıra urgency ve vajinal meş erozyonunu da minimal düzeyde tutmuştur.
\n
\n
\n